

LEADERSHIP EDUCATION AND TRAINING
Health-promoting leadership as a core competency across the physician leadership education spectrum
![]()
Victor Do, MD
Physicians are increasingly expected to lead teams, programs, and health care systems in contexts marked by growing clinical complexity, workforce distress, and persistent inequities. In response, physician leadership education has expanded across the education and career continuum; yet, well-being is often addressed as a parallel concern rather than as a core leadership responsibility. This article advances health-promoting leadership as a framework for understanding how leadership practices shape the conditions for health within medical learning and working environments. Informed by the Okanagan Charter and contemporary leadership scholarship, this article conceptualizes health-promoting leadership as a core, teachable competency that can guide physician leadership education. It describes key competency domains; outlines how health-promoting leadership can be cultivated across stages of training and practice; and identifies institutional responsibilities for aligning leadership education, governance, and accountability with the creation of healthy, equitable, and sustainable health care environments.
KEY WORDS: health promotion, leadership education, Okanagan Charter
Do V. Health-promoting leadership as a core competency across the physician leadership education continuum. Can J Physician Leadersh 12(1): 31-42. https://doi.org/10.37964/cr24804
Over the past decade, physician leadership education has gained increasing prominence across undergraduate, postgraduate, and continuing professional development contexts. Leadership programs commonly address domains, such as change management, quality improvement, negotiation, and organizational governance, reflecting the growing recognition that physicians play influential roles within health care systems.1 At the same time, physician burnout, moral distress, and workforce strain have been widely identified as pressing challenges with implications for health care quality, system sustainability, and patient safety.2
These parallel developments have created an important opportunity to examine more closely the relation between leadership and health in medical learning and working environments. Leadership is increasingly understood as shaping not only organizational performance, but also the everyday conditions in which physicians learn, work, and provide care. Decisions related to workload, team functioning, communication, and resource allocation influence psychological safety, trust, and well-being, and they accumulate over time to shape professional identity, team culture, and system sustainability.3 Leadership practices, therefore, function as an important influence on health at individual, team, and system levels.
In many leadership curricula, well-being is addressed as a distinct or complementary topic, commonly through self-care strategies, resilience-building approaches, or optional wellness initiatives.1 Although these efforts are valuable, they may not fully capture the ways in which leadership practices and organizational structures actively shape health. Physician leaders are frequently encouraged to support well-being without explicit attention to how leadership itself functions as a mechanism through which health is promoted or undermined in clinical and educational environments.
The Okanagan Charter4 offers a useful and underused framework for addressing this gap in physician leadership education. The charter articulates interrelated action areas that emphasize embedding health into institutional culture, fostering health-promoting environments, supporting personal and collective well-being, promoting community engagement, advancing research and scholarship, and aligning leadership and governance with health promotion. Although developed for academic institutions, the charter’s principles align closely with the realities of medical education and health care organizations, where leadership decisions shape learning environments, workplace culture, and the conditions for health.
Health-promoting leadership provides a way to translate the Okanagan Charter’s strategic directions into leadership education and practice. By emphasizing how leadership practices influence environments, relationships, and systems of care, health-promoting leadership positions well-being as an outcome of intentional leadership action rather than an individual responsibility alone. In this article, we explore how health-promoting leadership, informed by the Okanagan Charter, can guide physician leadership education across the continuum of training and practice.
Defining health-promoting leadership in medicine
Health-promoting leadership can be defined as leadership practice that intentionally creates, sustains, and repairs the conditions that enable psychological, social, and organizational health.5 Rather than focusing narrowly on individual well-being interventions, health-promoting leadership attends to how culture, power, relationships, policies, and learning environments shape health outcomes for learners, clinicians, and patients. This framing shifts attention from individual coping to the broader institutional and relational contexts in which health is produced.
In medical contexts, health-promoting leadership is enacted through everyday leadership actions. This includes how leaders structure work and learning environments; respond to error, uncertainty, and vulnerability; and distribute power, voice, and recognition within teams. It also encompasses how leaders address inequities embedded in systems and practices, and how they align stated values with operational decisions. These leadership practices directly shape whether clinical and educational environments foster trust, psychological safety, and belonging or contribute to distress, disengagement, and moral injury.
The Okanagan Charter provides a useful lens for conceptualizing these leadership actions. It has been adapted to the medical context to emphasize creating supportive environments, integrating health into organizational culture, and aligning leadership and governance with health promotion.6 Health-promoting leadership operationalizes these principles by translating them into leadership competencies that can be taught, practised, and evaluated in medical education and leadership training programs.
Health-promoting leadership is distinct from traditional leadership competencies. It does not replace skills, such as strategic planning or financial stewardship. Instead, it reframes their purpose by recognizing that decisions related to efficiency, performance, and change carry consequences for health. Within this orientation, leaders are accountable not only for organizational outcomes, but also for the health effects of the environments they create.
Health-promoting leadership is not synonymous with wellness programming. It represents an ethical orientation to leadership practice that recognizes leadership as a mechanism through which health is either produced or eroded within health care systems. By making these dynamics explicit, health-promoting leadership offers a foundation for physician leadership education that aligns closely with the Okanagan Charter’s vision of institutions as settings that actively promote health.
Why health-promoting leadership must be developed across the continuum
Leadership identity and leadership practice are often shaped before physicians assume formal leadership titles.7 From the earliest stages of training, physicians are exposed to implicit and explicit messages about authority, hierarchy, endurance, and professionalism through role modeling and the hidden curriculum.8 How supervisors respond to mistakes, how clinical workload is justified or normalized, and how learner vulnerability is acknowledged or dismissed all function as powerful lessons about leadership. These experiences contribute to deeply ingrained assumptions about whose well-being matters, how power should be exercised, and what forms of behaviour are rewarded in medical environments.
When health-promoting leadership is introduced only in mid- or late-career leadership programs, physicians may already have internalized leadership norms. In contrast, leadership education that explicitly names leadership as a determinant of health from the outset supports physicians in recognizing their influence across a range of contexts, including situations in which they do not hold formal authority. Embedding health-promoting leadership across the physician education and career continuum supports coherence among what physicians are taught in formal curricula, what they observe in clinical settings, and what they are ultimately expected to enact as leaders.
Core competency domains for health-promoting leadership
To meaningfully integrate health-promoting leadership into physician leadership education, programs must move beyond aspirational language and articulate clear, teachable competency domains. Without explicit competencies, leadership education risks positioning health and well-being as values rather than as skills that can be developed, practised, and evaluated. The Okanagan Charter provides a useful organizing framework for this work. Drawing on these principles, here are five proposed interrelated competency domains that should be intentionally embedded across leadership curricula and revisited at various stages of the physician education and career continuum.
1. Creating healthy learning and working environments
Health-promoting physician leaders require the ability to recognize how organizational structures, policies, and workflows shape health in learning and care environments. This includes understanding how workload design, scheduling practices, supervisory expectations, and evaluation systems influence psychological safety, chronic stress, and sustainability over time. Leadership education should support physicians in developing the capacity to identify environmental contributors to distress and disengagement, rather than attributing challenges solely to individual limitations. This domain closely aligns with the Okanagan Charter’s emphasis on creating supportive and health-promoting environments by equipping leaders with systems-thinking skills and the ability to redesign processes in ways that promote learning, recovery, and long-term workforce sustainability rather than endurance alone.
2. Relational leadership and trust stewardship
Trust is foundational to effective leadership and to the functioning of healthy clinical teams. Health-promoting leadership involves the capacity to build, maintain, and repair trust, particularly in contexts characterized by uncertainty, conflict, or harm. Physician leaders must be prepared to attend to how trust is influenced by transparency, consistency, follow-through, and responsiveness to concerns raised by learners and colleagues. Leadership education in this domain should address how trust is strengthened or eroded through everyday interactions, including how leaders communicate during crises, respond to feedback, and acknowledge mistakes. This competency reflects the Okanagan Charter’s focus on fostering supportive institutional cultures and strengthening relationships as a core mechanism through which health is promoted.
3. Power, equity, and inclusion in leadership practice
Leadership decisions inevitably shape how power, burden, and opportunity are distributed in health care environments. Health-promoting leaders must be able to recognize how power operates within teams and institutions and how structural inequities influence experiences of safety, belonging, and voice. Leadership education should move beyond a narrow focus on individual bias to examine how policies, norms, and leadership practices can either perpetuate or disrupt inequity. This includes supporting leaders to reflect on whose perspectives are prioritized, whose labour is rendered invisible, and how decisions may differentially affect learners and staff from structurally marginalized groups. This domain aligns with the Okanagan Charter’s commitment to equity, diversity, and social justice as foundational to health-promoting institutions.
4. Modeling vulnerability and psychological safety
Physician leaders play a critical role in shaping whether vulnerability is perceived as a professional risk or as a foundation for learning and growth. Health-promoting leadership includes modeling uncertainty, reflection, and accountability, and responding to error in ways that support improvement rather than fear or blame. Leadership education should explicitly address how leaders’ responses to mistakes, questions, and expressions of distress signal what is safe to say and do within teams. By learning to model vulnerability appropriately and to foster psychological safety, physician leaders can create environments that support open communication, learning, and collective responsibility. This competency reflects the Okanagan Charter’s emphasis on cultivating cultures that support well-being and enable individuals and communities to thrive.
5. Accountability for health and well-being outcomes
Health-promoting leadership ultimately requires accountability. Physician leaders should be trained to consider health and well-being outcomes as meaningful indicators of leadership effectiveness, alongside traditional metrics related to productivity, efficiency, and performance. This includes the ability to interpret data related to workforce well-being, learning environment quality, and equity, and to integrate these considerations into strategic and operational decision-making. Leadership education in this domain aligns with the Okanagan Charter’s call to align leadership, governance, and institutional priorities with health promotion. This shift moves leadership education from supporting well-being as an ancillary concern to accepting responsibility for the conditions that produce health within systems, reinforcing health-promoting leadership as a core leadership function rather than an optional commitment.
Teaching health-promoting leadership across the continuum
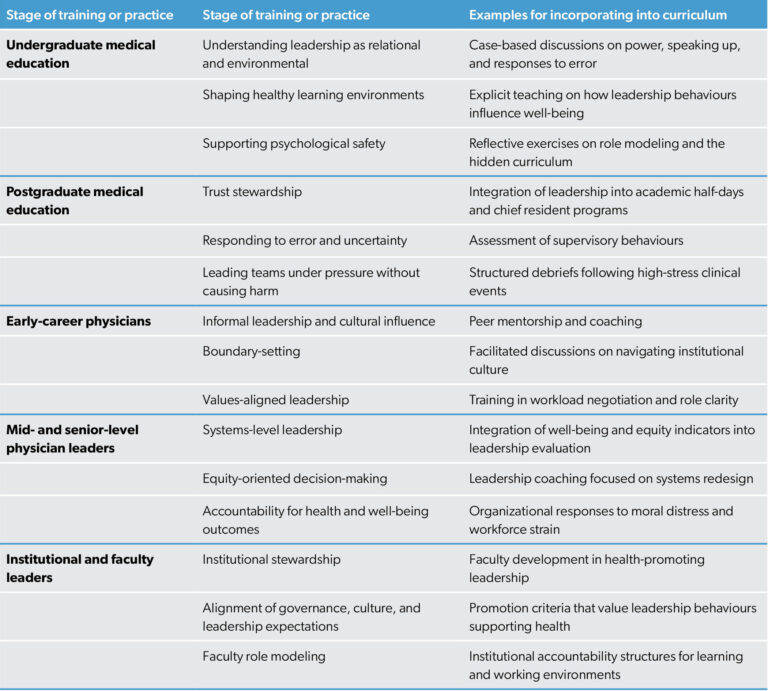
The Okanagan Charter emphasizes that health promotion must be embedded across institutional roles, structures, and stages of engagement, rather than addressed through isolated or time-limited interventions. Teaching health-promoting leadership through the lens of the Okanagan Charter encourages educators to align leadership education with the creation of supportive environments, the integration of health into institutional culture, the advancement of equity, and the alignment of leadership and governance with health promotion. Table 1 provides a summary of the health promoting leadership competencies that can be prioritized at different stages of physician training and practice.
Undergraduate medical education: foundations and identity formation
In undergraduate medical education, leadership is often framed as a future responsibility associated with formal roles, rather than as a set of everyday practices enacted through interactions, teamwork, and responses to challenge. Health-promoting leadership education offers an opportunity to reframe leadership as something that is exercised daily, even by those without positional authority, and to situate leadership within the stewardship of learning and care environments. This approach aligns with the Okanagan Charter’s call to embed health into institutional culture from the earliest points of engagement.
Educational approaches at this stage should introduce leadership early as a responsibility for shaping healthy learning environments and relationships. Case-based discussions can be used to examine power dynamics, speaking up, and responses to error, supporting learners in recognizing how leadership behaviours influence psychological safety, trust, and belonging. Explicitly naming leadership practices that promote or undermine health helps learners develop a shared language for discussing leadership and well-being, reinforcing the idea that health is produced through everyday interactions and institutional norms. The central shift in undergraduate education is from viewing leadership as positional to understanding it as relational and environmental, thereby embedding health-promoting leadership within early professional identity formation.
Postgraduate medical education: applied leadership and role modeling
During residency and fellowship, physicians occupy dual roles as learners and supervisors, making this a critical period for applied leadership development. Health-promoting leadership education at this stage should emphasize skill-building through lived experience and role modeling, as residents’ leadership behaviours have immediate consequences for team functioning, learning environments, and patient care. The ways in which residents lead rounds, manage uncertainty, and respond to error communicate powerful messages about professionalism, safety, and whose well-being matters within clinical settings.
Leadership education in postgraduate training should integrate health-promoting leadership principles into existing structures, such as academic half-days, leadership curricula, and chief resident programs. Leadership behaviours that support psychological safety, equity, and learning should be recognized and assessed as part of supervisory roles, reinforcing their importance alongside clinical competence. Training should also prepare residents to lead teams during high-stress clinical situations in ways that preserve trust and minimize harm. This approach reflects the Okanagan Charter’s emphasis on creating supportive environments and strengthening institutional capacity for health promotion.
Early-career physicians: informal leadership and cultural influence
Early-career physicians can exert substantial influence within teams and organizations despite lacking formal leadership titles. Leadership education at this stage should acknowledge and support this reality by focusing on informal leadership, cultural influence, and boundary-setting. As new staff physicians navigate institutional expectations and entrenched norms, they frequently encounter tensions between personal values and prevailing practices, particularly in relation to workload, availability, and definitions of professionalism.
Health-promoting leadership education for early-career physicians should address navigating institutional cultures, setting boundaries around workload, and negotiating roles and expectations in ways that align with health-promoting values. Supporting physicians in understanding their influence as culture carriers can help them engage more intentionally in shaping team norms and practices, even in the absence of formal authority. This approach aligns with the Okanagan Charter’s emphasis on empowering individuals and communities to take action for health.
Mid- and senior-level physician leaders: systems and accountability
For physicians in formal leadership roles, health-promoting leadership education must address systems-level accountability. At this stage, leaders have significant influence over policies, resource allocation, and institutional priorities, all of which shape the health of learning and working environments. Leadership education should, therefore, equip leaders to recognize the health implications of strategic and operational decisions and to understand how leadership and governance structures can either support or undermine institutional commitments to well-being and equity.
Programs for mid- and senior-level physician leaders should integrate well-being and equity indicators into leadership evaluation, planning, and decision-making processes. Leaders should be supported in aligning operational choices with health-promoting values and in addressing moral injury and distress at a systems level rather than through individual remediation alone. This approach reflects the Okanagan Charter’s call to align leadership and governance with health promotion and represents a central shift from managing burnout reactively to designing systems that proactively promote health.
Institutional responsibilities for advancing health-promoting leadership
Embedding health-promoting leadership into physician education cannot rely solely on individual programs or local champions. Institutions play a critical role in shaping the conditions under which leadership education is designed, delivered, and valued. The Okanagan Charter explicitly calls on institutions to align leadership and governance with health promotion, emphasizing that health-promoting environments require structural commitment rather than discretionary effort.
Institutions must recognize health-promoting as a core leadership competency and signal its importance through formal expectations, evaluation processes, and accountability structures. Leadership training should be aligned with promotion and performance frameworks so that leadership behaviours that support health, equity, and psychological safety are valued alongside traditional indicators of success. Investment in faculty development is also essential, as educators and clinical leaders serve as powerful role models whose everyday practices shape the hidden curriculum of leadership. Without institutional alignment, leadership education risks reinforcing the very conditions that contribute to distress, inequity, and disengagement within medical learning and working environments.
Limitations
This viewpoint is conceptual in nature and does not present empirical evaluation of health-promoting leadership education or outcomes. Although the Okanagan Charter offers a robust and transferable framework, its application to physician leadership education may require contextual adaptation across institutions, specialties, and health system settings. In addition, the competency domains and educational approaches described reflect a synthesis of existing scholarship and practice rather than a prescriptive model. Future empirical work is needed to evaluate how health-promoting leadership education influences leadership behaviours, learning and working environments, and health outcomes across the physician education and career continuum.
Conclusion: from leadership training to leadership responsibility
Health-promoting leadership offers an important reframing of physician leadership education. By recognizing leadership as a determinant of health, educators and institutions can move beyond preparing physicians to cope within unhealthy systems toward equipping them to actively shape healthier learning and care environments. Grounded in the principles of the Okanagan Charter, this approach positions leadership education as a form of health promotion that operates through culture, relationships, and governance. Embedding health-promoting leadership as a core competency across the physician education and career continuum positions leadership education as a powerful lever for cultural and systems change.
References
- Lott GL, Pyzdrowski DM, Araya B, Tiryaki E, Zagoloff A, Prasad S, et al. Physician leadership programs: a literature review. Leadersh Health Serv 2026;39(1):44-56. https://doi.org/10.1108/LHS-05-2025-0073
- Dyrbye LN, Shanafelt TD, Sinsky CA, Cipriano PF, Bhatt J, Ommaya A, et al. Burnout among health care professionals: a call to explore and address this underrecognized threat to safe, high-quality care. NAM Perspectives 2017;5 Jul. https://doi.org/10.31478/201707b
- Spilg EG, McNeill K, Dodd-Moher M, Dobransky JS, Sabri E, Maniate JM, et al. Physician leadership and its effect on physician burnout and satisfaction during the COVID-19 pandemic. J Healthc Leadersh 2025;17:49-61. https://doi.org/10.2147/JHL.S487849
- Okanagan Charter: an international charter for health promoting universities and colleges. 2015. Available: https://open.library.ubc.ca/media/stream/pdf/53926/1.0132754/7
- Do V, Lewis M, Flynn L, Sonnenberg LK. Sick by design? Why medical education needs health promoting learning environments. Can Med Educ J 2025;16(1):123. https://doi.org/10.36834/cmej.80471
- Do V, Lewis M, Goldstein C, Sonnenberg LK. Fostering a health-promoting learning environment in medical education: adapting the Okanagan Charter for administrators and medical educators. Acad Med 2023;98(6):672-9.
https://doi.org/10.1097/ACM.0000000000005159 - Quinn JF, Perelli S. First and foremost, physicians: the clinical versus leadership identities of physician leaders. J Health Organ Manage 2016;30(4):711-28. https://doi.org/10.1108/JHOM-05-2015-0079
- Hafferty FW, Castellani B. The hidden curriculum: a theory of medical education. In Brosnan C, Turner BS (editors). Handbook of the sociology of medical education. Abingdon-on-Thames, U.K.: Routledge; 2009: p. 15-35.
Author
Victor Do, MD, FRCPC, is a pediatric hospital medicine physician at Stollery Children’s and Glenrose Rehabilitation Hospitals and a clinical lecturer in the Department of Pediatrics, University of Alberta.
Funding: No funding is associated with this article.
Conflicts of interest: The author has no relevant conflicts of interest to declare.
Correspondence to:
Vdo@ualberta.ca