![]()
 Background: Canadian pathologists lack workload protection, resulting in excessive unpaid overtime, which contributes to medical errors, rising medicolegal risk, and mental health deterioration. This crisis has resulted in repeated public inquiries about quality of patient care.
Background: Canadian pathologists lack workload protection, resulting in excessive unpaid overtime, which contributes to medical errors, rising medicolegal risk, and mental health deterioration. This crisis has resulted in repeated public inquiries about quality of patient care.
KEY WORDS: pathology, workload, burnout, workforce, well-being, psychological security
Maung R, Bonert M, Soll B, Dow H. Canadian pathologists in crisis: a review of national well-being and workload data. Can J Physician Leadersh 2025;11(3): 120-130. https://doi.org/10.37964/cr24795
Method: This study is a general review of national data with an observational component. First, we correlated workforce-to-population ratio with medicolegal burden. Second, we used Canadian Medical Association (CMA) wellness survey data to rank pathology against other specialties in terms of 17 wellness indicators.
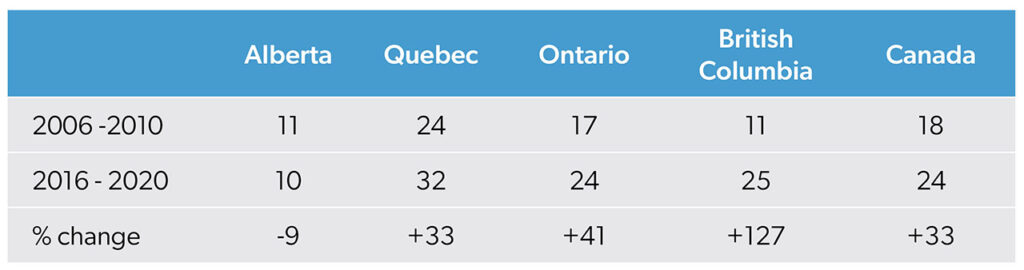
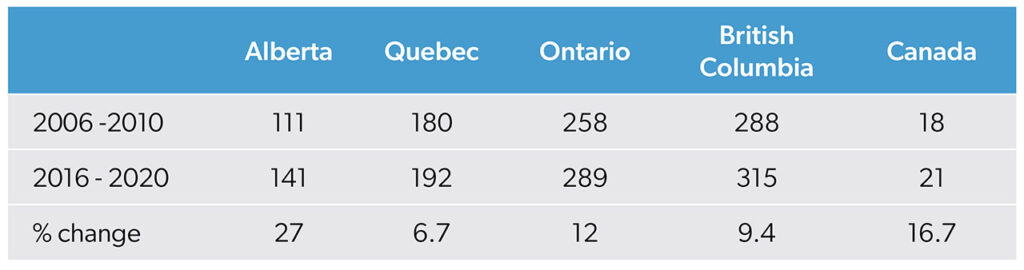
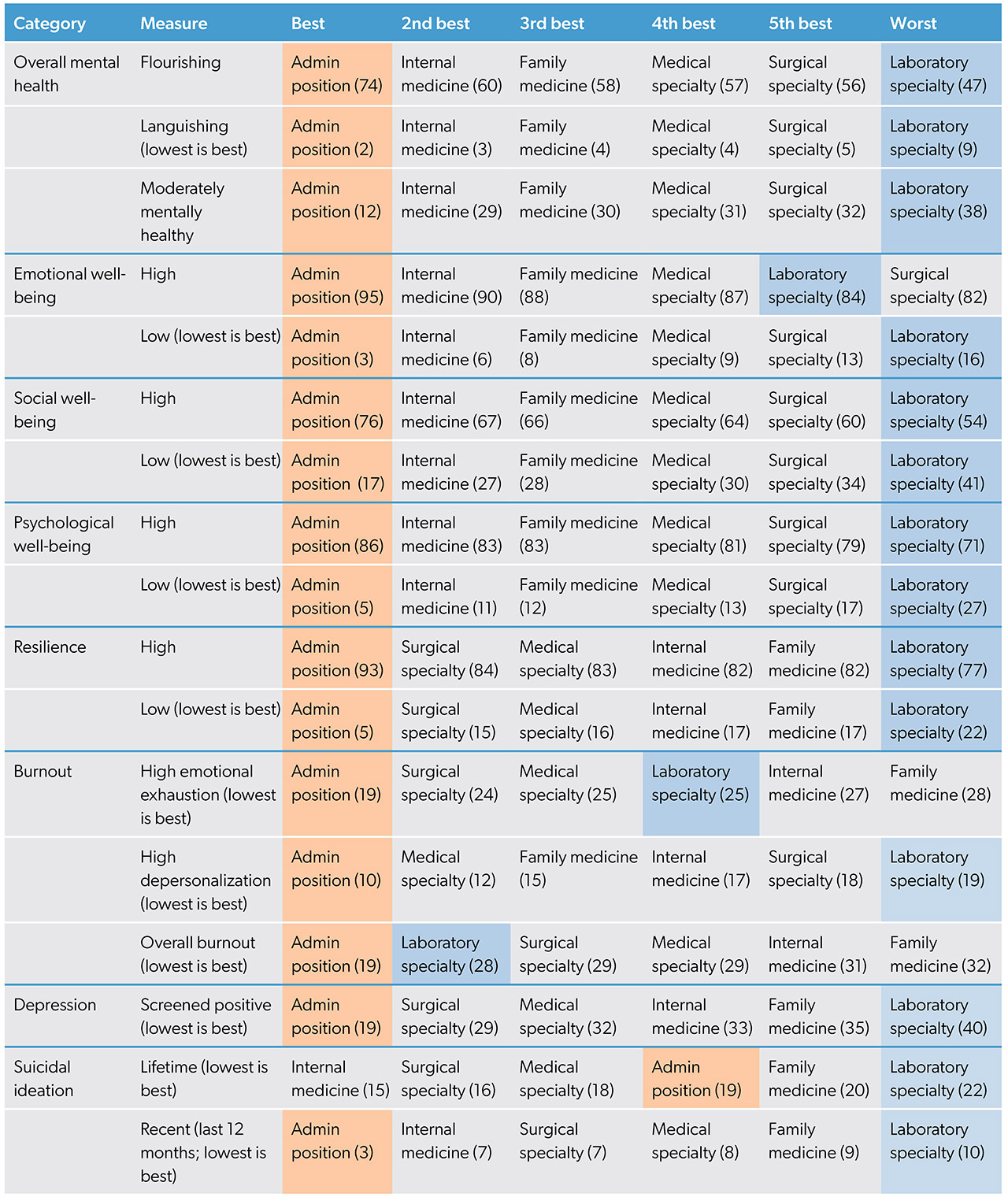
Results: From 2006–2010 to 2016–2020, medicolegal cases per pathologist rose disproportionately. This was most evident in British Columbia (127% increase in complaints vs. 9.4% growth in workforce) and Ontario (39% vs. 15%). Nationally, complaints rose 33% vs. a 16.7% workforce increase. In contrast, Alberta, with the highest workforce growth (27%), saw a 9% decline in complaints. Pathologists ranked worst on 14 of 17 wellness indicators in the 2018 CMA wellness survey. They reported the lowest levels of psychological well-being and the highest rates of distress. Pathologists had a 2.44-fold increased risk of low psychological well-being compared with physicians in other specialties.
Interpretation: The pathology workforce crisis is driven by excessive workload, inadequate structural support, and rising medicolegal scrutiny, which collectively erode well-being. Addressing these issues requires systemic reform, workload-based contracts, and mental health protections to sustain both physician wellness and patient care quality.
Pathologists strive to deliver the highest quality of patient care. The precision and quality of that care are improving — medicine’s evolving knowledge base has enabled meticulous management of complex cases, ancillary studies have expanded, and reporting requirements have become more rigorous.1,2 Despite their increased workload, pathologists do the best that they can — until they no longer can. Currently, Canadian pathologists face an employment model that is unique in Canadian medicine; it lacks workload protections and forces them into excessive unpaid overtime without contractual safeguards. This contributes to rising medicolegal risk and deteriorating mental health.
Laboratories face unpredictable specimen volumes, making workload management difficult. A study analyzing pathology reports from 2011 to 2019 found that, despite a 6% decrease in total cases per year, the workload of pathologists increased substantially: 20% more “blocks,” 23% more workload units, and 19% more report lines.1 This was matched by only a 1% increase in the workforce.1 Unlike that of fee-for-service physicians, pathologists’ workload is not tied to compensation. Hospitals have little incentive to pay for overtime, leading to prioritization of increased output from existing staff rather than hiring additional pathologists.3
Unionization is illegal in most provinces, and Ontario’s Employment Standards Act4 excludes physicians, leaving salaried and contracted pathologists without labour protections. As a result, pathologists must manage overwhelming workloads without mechanisms to redistribute cases or advocate improved conditions. These demands, coupled with systemic neglect, contribute to severe professional distress.
Unsurprisingly, Canadian pathologists experience some of the worst mental health outcomes in the Canadian medical profession.5 A pre-pandemic study found burnout rates among Canadian pathologists of 57.7%6 — exceeding the 35–40% reported among American pathologists who operate under a fee-for-service model.7 Lack of workload control is a primary driver of burnout and disengagement among pathologists8 and is associated with increased medical errors and higher medicolegal exposure.9 Excessive workloads and task maldistribution also contribute to staff absences and departures, further straining the remaining workforce1,8 and damaging morale.
This study presents a national-level review of workforce data. Its primary objective is to examine the relation between the Canadian pathologist workforce and medicolegal risk over time. A secondary objective is to compare the well-being indicators of pathologists with those of other medical specialties.
Method
Design
We carried out a general review using an observational approach. Because of the lack of a unified national dataset linking workforce data with medicolegal cases, we aggregated independent datasets. To our knowledge, these are the only national datasets covering the pathology workforce, medicolegal trends, and physician wellness in Canada.
We conducted two independent analyses: the relation between workforce and medicolegal complaints; and the well-being of pathologists compared with other specialties.
Data sources
To study the relation between workforce and medicolegal complaints, we looked at data from the Canadian Institute for Health Information.10 Workforce data included the number of pathologists per 100 000 population, specialty, and province. For statistical reasons, only large provinces (British Columbia, Alberta, Ontario, Quebec, and Canada as a whole) were included. Specialties included in the analysis were anatomical pathology, general pathology, hematological pathology, and neuropathology.
On our request, the Canadian Medical Protective Association (CMPA) provided data on self-reported medicolegal cases of its members by province and specialty. The 2006–2010 and 2016–2020 periods provided by the CMPA dictated the periods included in the analysis. Data included civil complaints, college complaints, and hospital complaints.
For the second study, pathologists’ well-being, we examined the CMA National Physician Health Survey (2018),5 which included mental health data, such as burnout and workplace stressors, with laboratory specialty-specific findings. The 2021 survey11 did not separately identify lab specialists, making the 2018 survey the most recent dataset.
Analysis
An observational analysis explored the relation between the number of practising pathologists per 100 000 population and medicolegal complaints per 1000 members of the CMPA, by region. Because of the limited number of cases, data were aggregated into two five-year periods. Aggregation was performed by averaging workforce numbers and medicolegal cases within each period. These values were not normalized further. Given that both datasets were independent and confounders could not be controlled, the analysis remained descriptive and exploratory. The relation between workforce changes and medicolegal case volumes was assessed using Spearman’s rank correlation coefficient.
Mental health rankings by specialty were determined using 17 wellness indicators from the CMA 2018 National Physician Health Survey.5 Each specialty was ranked best to worst based on flourishing mental health, emotional well-being, burnout, and depression screening positivity. Positive indicators (e.g., psychological well-being) were ranked in descending order, while negative indicators (e.g., burnout, suicidal ideation) were ranked in ascending order. Because of the lack of access to raw data, sensitivity analyses were not possible.
Ethics approval
As all data were either publicly available (CIHI, CMA) or available on request from the controlling organizations (CMPA), this study did not require ethics approval under institutional and national research ethics guidelines.9
Results
During the study period, medicolegal complaints rose by 33% (Table 1), far outpacing workforce growth (Table 2), suggesting an escalation of the burden per pathologist. A Spearman’s rank correlation (rS(3) = −0.56, p = 0.322) indicated a moderate negative correlation, suggesting that as workforce grew, medicolegal cases increased disproportionately per pathologist. This trend was most pronounced in British Columbia (127% increase in complaints compared with a 9.4% increase in workforce) and Ontario (41% increase in complaints compared with a 12% increase in workforce). This trend was opposite in Alberta, where a 27% increase in workforce was accompanied by a 9% decrease in complaints.